November 2022
Produce Prescription programs (PRx) are gaining national attention, and a long-sought after chance to be embedded into national policy - the White House National Strategy on Hunger, Nutrition and Health defines the objective to “Expand Medicare and Medicaid beneficiaries’ access to “food is medicine” interventions,” including PRx specifically (1). This is a very exciting moment, one that many of us have worked hard to accomplish. But there is also a tension between what is included in PRx, and what will be the policy that is embedded as it moves forward.
| I had the privilege of working closely with August (Gus) Schumacher for a few years at Wholesome Wave, the organization he co-founded, and before that counted him as a friend and mentor for many more years. In our time together, we visited many farmers’ markets, across numerous states, and in a variety of low-income urban and rural communities. Gus would visit each stand at the market, chatting, tasting, and schmoozing with each farmer. Almost invariably, Gus knew a number of farmers at these markets, often knew their family going back a couple generations, inquiring about parents and cousins. Gus didn’t only know farmers, he often also knew local public officials, veterans moving through in wheelchairs, local journalists, and nearby health clinic leaders, from his many visits over the years. |  |
Gus took great joy in the mix of people that were at the farmers’ markets and the market day buzz of community activity. He greeted everyone, farmers, customers, people out in the market area, and asked all their opinions with equal gravity.
Gus’ accomplishments are legendary, he served as Under-Secretary of Agriculture during the Clinton Administration, established WIC farmers’ market coupons, was Massachusetts Commissioner of Agriculture to name a few. USDA’s August Schumacher Nutrition Incentive Program (GusNIP) funding program is named after him due to his innovations and tireless promotion of nutrition incentives as a consummate leader and connector. But what I most learned from and loved was his gift that was to include everyone, talk to everyone, make all feel known and recognized for their contributions, always listening. The input he received walking and chatting at farmers markets was integrated into real national policy.
While Gus was not the originator of the Produce Prescription (PRx) program model, he understood its power to make connections, and helped to make Wholesome Wave an early pioneer and driver in the field. The Wholesome Wave models consisted of pediatricians at community health clinics “prescribing” healthy produce to patient families where there was risk of diabetes, with the prescriptions redeemable at a local farmers’ market.
Gus’ accomplishments are legendary, he served as Under-Secretary of Agriculture during the Clinton Administration, established WIC farmers’ market coupons, was Massachusetts Commissioner of Agriculture to name a few. USDA’s August Schumacher Nutrition Incentive Program (GusNIP) funding program is named after him due to his innovations and tireless promotion of nutrition incentives as a consummate leader and connector. But what I most learned from and loved was his gift that was to include everyone, talk to everyone, make all feel known and recognized for their contributions, always listening. The input he received walking and chatting at farmers markets was integrated into real national policy.
While Gus was not the originator of the Produce Prescription (PRx) program model, he understood its power to make connections, and helped to make Wholesome Wave an early pioneer and driver in the field. The Wholesome Wave models consisted of pediatricians at community health clinics “prescribing” healthy produce to patient families where there was risk of diabetes, with the prescriptions redeemable at a local farmers’ market.
 | Gus saw and evangelized the elegance of the many connections and benefits of the model - patients eating healthier foods, doctors activated to support their patient’s full health, positioning of farmers as core providers of health for their communities, and a new flow of “prescription” dollars from the health sector that helped drive traffic and revenues for the markets and farmers themselves. |
Gus was not alone in his excitement about these holistic connections. Food, farm, and health activists around the country have helped to establish over 90 PRx programs throughout the country (2021 PRx Field Scan, Link Here ), and the USDA August Schumacher Nutrition Incentive Program (GusNIP) funding and supporting dozens more to emerge. In the recent White House Conference on Hunger… commitment to Food as Medicine, calls for multiple federal policies supporting PRx:
| Expand Medicare and Medicaid beneficiaries’ access to “food is medicine” interventions. “Food is medicine” interventions—including medically tailored meals and groceries as well as produce prescriptions (fruit and vegetable prescriptions or vouchers provided by medical professionals for people with diet-related diseases or food insecurity)—can effectively treat or prevent diet-related health conditions and reduce food insecurity. And to: Increase access to nutrition-related services through private insurance and federal programs beyond Medicare and Medicaid. |
PRx programs have evolved to utilize a variety of redemption venues, including supermarkets, and home-delivered veggie boxes, and are now active in multiple clinical settings. Now some PRx programs no longer have any redemption with local farmers, entirely utilizing card-based technologies with chain retailers.
As PRx programs have begun to grow around the country, and have shown many positive health impacts, many leaders are working on getting them institutionalized into state and federal policies. There has been some early success in the Produce Prescription funding included in USDA GusNIP competitive grants program, but the ultimate goal seems to be development of a new PRx benefit within Medicaid and Medicare systems.
| “Advancing federal and state policy change that leverages Produce Prescriptions as prevention & intervention for diet-related disease and further embeds this effective model into healthcare and food retail systems. The current goal of the NPPC is to make produce prescriptions a covered benefit for all eligible patients covered by Medicaid & Medicare” - National Produce Prescription Collaborative |
In spite of a unified shift to scale PRx programs as a response to health disparities, within this pursuit of health-focused policy, a tension has arisen between food & farm program leaders, and health-focused leaders.
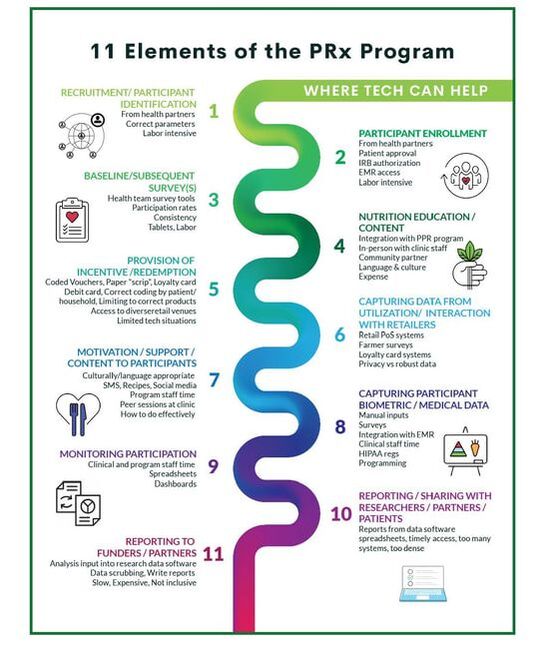
Some (not all) PRx program leaders working on policy change make the case that in order to be successful embedding PRx into healthcare systems, it must be entirely seen as a healthcare intervention, and what we need are efficient systems to deliver this intervention and impact data, to impress on healthcare policy makers that this intervention is scalable and cost effective. They emphasize standardization of data and systems to allow for the biggest data sets possible to show impacts. In this approach, farmers’ markets are largely set aside as too complex and inconvenient as the primary design for redemption venues, as are smaller neighborhood stores (such as bodegas, corner stores, ethnic grocery stores, etc), lacking consistent technology and capacity. These leaders ultimately want large retailers and health systems to integrate PRx programs, with community-based organizations being phased out as activators and managers.
I have heard some (not all) PRx program leaders focused on embedding into health say that any advocacy or program design around food & farm systems or local farmers is only distracting and even disruptive to the primary goal of health adoption.
Other activists continue to focus on a more holistic approach - that local food & farmers are important for long-term community health. Some Black Indigenous and People of Color (BIPOC) leaders have emphasized the importance of cultural foods, investment of the prescription dollars in BIPOC-owned producers and retailers, dignified farmers and local food systems jobs. They see the ethnic grocery stores, bodegas, co-ops, and markets of their communities as key assets to support. They have their prescriptions redeemable at urban and rural markets owned by community members, sometimes still resorting to paper coupons when technology is not available for these lower-resourced retailers.
Knowing the many obstacles low-income patients face, many community-driven programs add-in wrap around supports to make the program accessible and effective. These programs make sure to provide cultural healthy recipes and ongoing appropriate motivations to patients from community health workers. They provide culturally-centered nutrition education and fun incentives to participate. They support and build new distribution and retail assets where they are lacking. They take into consideration the transportation issues that low-income people often face, and use creative solutions like home-delivery and mobile markets to bring healthy food right to isolated patients, understanding the unique needs of their home communities.
Some (not all) PRx program leaders working on policy change make the case that in order to be successful embedding PRx into healthcare systems, it must be entirely seen as a healthcare intervention, and what we need are efficient systems to deliver this intervention and impact data, to impress on healthcare policy makers that this intervention is scalable and cost effective. They emphasize standardization of data and systems to allow for the biggest data sets possible to show impacts. In this approach, farmers’ markets are largely set aside as too complex and inconvenient as the primary design for redemption venues, as are smaller neighborhood stores (such as bodegas, corner stores, ethnic grocery stores, etc), lacking consistent technology and capacity. These leaders ultimately want large retailers and health systems to integrate PRx programs, with community-based organizations being phased out as activators and managers.
I have heard some (not all) PRx program leaders focused on embedding into health say that any advocacy or program design around food & farm systems or local farmers is only distracting and even disruptive to the primary goal of health adoption.
Other activists continue to focus on a more holistic approach - that local food & farmers are important for long-term community health. Some Black Indigenous and People of Color (BIPOC) leaders have emphasized the importance of cultural foods, investment of the prescription dollars in BIPOC-owned producers and retailers, dignified farmers and local food systems jobs. They see the ethnic grocery stores, bodegas, co-ops, and markets of their communities as key assets to support. They have their prescriptions redeemable at urban and rural markets owned by community members, sometimes still resorting to paper coupons when technology is not available for these lower-resourced retailers.
Knowing the many obstacles low-income patients face, many community-driven programs add-in wrap around supports to make the program accessible and effective. These programs make sure to provide cultural healthy recipes and ongoing appropriate motivations to patients from community health workers. They provide culturally-centered nutrition education and fun incentives to participate. They support and build new distribution and retail assets where they are lacking. They take into consideration the transportation issues that low-income people often face, and use creative solutions like home-delivery and mobile markets to bring healthy food right to isolated patients, understanding the unique needs of their home communities.
| These community-driven programs are leveraging their precious program dollars to make recirculating investments into not only immediate individual patient health improvements, but into the longer-term healthy community environments. |  |
When programs focus only on scale and standardization of data, there are risks that the local nuances of language, culture, specific needs and strengths, and community leadership can be overlooked. When programs are defined only at the mass scale by the largest actors, opportunities to invest in diverse assets can be lost, and disparities maintained.
The great vision of targeting institutionalization of PRx into Medicaid/Medicare is highly laudable. If achieved it would provide access to healthy fruits & vegetables for millions of low-income people who are most in need. It is a worthy and powerful ambition that would take a certain amount of strategic pragmatism required to have success in this quest.
But who gets left out of this trajectory? Who keeps power and profits in this model? From everything we have learned about community health, is access to fruits & vegetables enough for behavior change and long-term sustained population wellbeing?
The great vision of targeting institutionalization of PRx into Medicaid/Medicare is highly laudable. If achieved it would provide access to healthy fruits & vegetables for millions of low-income people who are most in need. It is a worthy and powerful ambition that would take a certain amount of strategic pragmatism required to have success in this quest.
But who gets left out of this trajectory? Who keeps power and profits in this model? From everything we have learned about community health, is access to fruits & vegetables enough for behavior change and long-term sustained population wellbeing?
Do we need to remove integration with food systems change in order to have success with healthcare policy? Of course, if we are to have fresh produce to keep our bodies healthy, we need viable farms, at least somewhere. And if we want people to be able to afford healthy produce outside of government benefits we need flourishing local economies. Our health leaders are also growing in awareness that “Social Determinants of Health,” such as access to fresh produce and decent economic opportunities, are as critical to positive health outcomes for populations as access to medical attention.
Albert Einstein said that you cannot solve a problem with the same kind of thinking that created the issue in the first place. I worry that if we remove food & farm systems from the core understanding of the PRx model, we are replicating the same kind of reductionist approach that has made us one of the unhealthiest societies in the world, allowing disparities in health and community development to persist. If we pass a PRx policy into Medicaid/Medicare that is only designed for redemption at large scale retailers or technology solutions, only designed to address chronic disease and the biometric indicators of health, will we have missed a major opportunity for a strong systemic solution, one that provides healthy produce to those most in need but also ripples these purchase dollars into local healthy rural and urban economies and builds community strengths?
Gus Schumacher loved talking about overcoming the “lawyers” who sought to deny or restrict his new farmers’ market coupon programs at USDA, with legal and bureaucratic red tape. Gus knew there would always be pushback, and special interests opposing or co-opting positive initiatives, and, with allies, and did not back down from these struggles. He used this pushback as chances to engage in conversations and call for more new allies.
I am not trying to express that this is an either/or situation, a battle between health and food systems. Nor am I saying that health institutions and grocery retailers are bad, or not part of the solution. There are wonderful thoughtful champions coming from these entities as well. There are also many initiatives in the PRx field working at all scales to forge creative partnerships and impact public health outcomes through increased access to fruits and vegetables. We need innovation and growth in the field to ensure this model reaches as many people as possible.
This moment in our country feels like an opportunity to keep striving for policies that are inclusive and done right, that honor the diverse people that have made community food and health systems flourish. As Gus did, can we see the power of community venues, see and recognize the farmers, community-based leaders, and all stakeholders, make sure they are thoughtfully included in the policies that we advocate for?
Gus Schumacher loved talking about overcoming the “lawyers” who sought to deny or restrict his new farmers’ market coupon programs at USDA, with legal and bureaucratic red tape. Gus knew there would always be pushback, and special interests opposing or co-opting positive initiatives, and, with allies, and did not back down from these struggles. He used this pushback as chances to engage in conversations and call for more new allies.
I am not trying to express that this is an either/or situation, a battle between health and food systems. Nor am I saying that health institutions and grocery retailers are bad, or not part of the solution. There are wonderful thoughtful champions coming from these entities as well. There are also many initiatives in the PRx field working at all scales to forge creative partnerships and impact public health outcomes through increased access to fruits and vegetables. We need innovation and growth in the field to ensure this model reaches as many people as possible.
This moment in our country feels like an opportunity to keep striving for policies that are inclusive and done right, that honor the diverse people that have made community food and health systems flourish. As Gus did, can we see the power of community venues, see and recognize the farmers, community-based leaders, and all stakeholders, make sure they are thoughtfully included in the policies that we advocate for?
(1) https://www.whitehouse.gov/wp-content/uploads/2022/09/White-House-National-Strategy-on-Hunger-Nutrition-and-Health-FINAL.pdf












 RSS Feed
RSS Feed